
By James Nicholls and Paul Cairney, for the University of Stirling MPH and MPP programmes.
There are strong links between the study of public health and public policy. For example, public health scholars often draw on policy theories to help explain (often low amounts of) policy change to foster population health or reduce health inequalities. Studies include a general focus on public health strategies (such as HiAP) or specific policy instruments (such as a ban on smoking in public places). While public health scholars may seek to evaluate or influence policy, policy theories tend to focus on explaining processes and outcomes.
To demonstrate these links, we present:
- A long-read blog post to (a) use an initial description of a key alcohol policy instrument (minimum unit pricing, adopted by the Scottish Government but not the UK Government) to (b) describe the application of policy concepts and theories and reflect on the empirical and practical implications. We then added some examples of further reading.
- A 45 minute podcast to describe and explain these developments (click below or scroll to the end)
Minimum Unit Pricing in Scotland: background and development
Minimum Unit Pricing for alcohol was introduced in Scotland in 2018. In 2012, the UK Government had also announced plans to introduce MUP, but within a year dopped the policy following intense industry pressure. What do these two journeys tell us about policy processes?
When MUP was first proposed by Scottish Health Action on Alcohol Problems in 2007, it was a novel policy idea. Public health advocates had long argued that raising the price of alcohol could help tackle harmful consumption. However, conventional tax increases were not always passed onto consumers, so would not necessarily raise prices in the shops (and the Scottish Government did not have such taxation powers). MUP appeared to present a neat solution to this problem. It quickly became a prominent policy goal of public health advocates in Scotland and across the UK, while gaining increasing attention, and support, from the global alcohol policy community.
In 2008, the UK Minister for Health, Dawn Primarolo, had commissioned researchers at the University of Sheffield to look into links between alcohol pricing and harm. The Sheffield team developed economic models to analysis the predicted impact of different systems. MUP was included, and the ‘Sheffield Model’ would go on to play a decisive role in developing the case for the policy.
What problem would MUP help to solve?
Descriptions of the policy problem often differed in relation to each government. In the mid-2000s, alcohol harm had become a political problem for the UK government. Increasing consumption, alongside changes to the night-time economy, had started to gain widespread media attention. In 2004, just as a major liberalisation of the licensing system was underway in England, news stories began documenting the apparent horrors of ‘Binge Britain’: focusing on public drunkenness and disorder, but also growing rates of liver disease and alcohol-related hospital admissions.

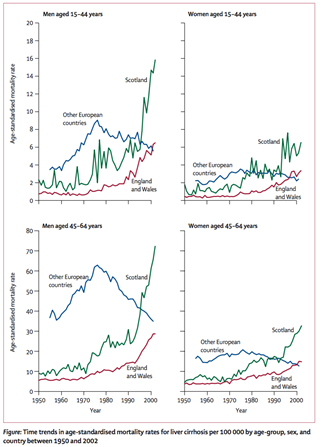
Politicians began to respond, and the issue became especially useful for the Conservatives who were developing a narrative that Britain was ‘broken’ under New Labour. Labour’s liberalising reforms of alcohol licensing could conveniently be linked to this political framing. The newly formed Alcohol Health Alliance, a coalition set up under the leadership of Professor Sir Ian Gilmore, was also putting pressure on the UK Government to introduce stricter controls. In Scotland, while much of the debate on alcohol focused on crime and disorder, Scottish advocates were focused on framing the problem as one of public health. Emerging evidence showed that Scotland had dramatically higher rates of alcohol-related illness and death than the rest of Europe – a situation strikingly captured in a chart published in the Lancet.
The notion that Scotland faced an especially acute public health problem with alcohol was supported by key figures in the increasingly powerful Scottish National Party (in government since 2007), which, around this time, had developed working relationships with Alcohol Focus Scotland and other advocacy groups.
What happened next?
The SNP first announced that it would support MUP in 2008, but it did not implement this change until 2018. There are two key reasons for the delay:
- Its minority government did not achieve enough parliamentary support to pass legislation. It then formed a majority government in 2011, and its legislation to bring MUP into law was passed in 2012.
- Court action took years to resolve. The alcohol industry, which is historically powerful in Scotland, was vehemently opposed. A coalition of industry bodies, led by the Scotch Whisky Association, took the Scottish Government to court in an attempt to prove the policy was illegal. Ultimately, this process would take years, and conclude in rulings by the European Court of Justice (2016), Scottish Court of Session Inner House (2016), and UK Supreme Court (2017) which found in favour of the Scottish Government.
In England, to the surprise of many people, the Coalition Government announced in March 2012 that it too would introduce MUP, specifically to reduce binge drinking and public disorder. This different framing was potentially problematic, however, since the available evidence suggested (and subsequent evaluation has confirmed) that MUP would have only a small impact on crime. Nonetheless, health advocates were happy, with one stating that ‘I do not mind too much how it was framed. What I mind about is how it measures up’.
Once again, the alcohol industry swung into action, launching a campaign led by the Wine and Spirits Trade Association, asking ‘Why should moderate drinkers pay more?’

This public campaign was accompanied by intense behind-the-scenes lobbying, aided by the fact that the leadership of industry groups had close ties to Government and that the All-Party Parliamentary Group on Beer had the largest membership of any APPG in Westminster. The industry campaign made much of the fact there was little evidence to suggest MUP would reduce crime, but also argued strongly that the modelling produced by Sheffield University was not valid evidence in the first place. A year after the adopting the policy, the UK Government announced a U-turn and MUP was dropped.
How can we use policy theories and concepts to interpret these dynamics?
Here are some examples of using policy theories and concepts as a lens to interpret these developments.
1. What was the impact of evidence in the case for policy change?
While public health researchers often expect (or at least promote) ‘evidence based’ policymaking, insights from research identify three main reasons why policymakers do not make evidence-based choices:
First, many political actors (including policymakers) have many different ideas about what counts as good evidence.
The assessment, promotion, and use of evidence is highly contested, and never speaks for itself.
Second, policymakers have to ignore almost all evidence to make choices.
They address ‘bounded rationality’ by using two cognitive shortcuts: ‘rational’ measures set goals and identify trusted sources, while ‘irrational’ measures use gut instinct, emotions, and firmly held beliefs.
Third, policymakers do not control the policy process.
There is no centralised and orderly policy cycle. Rather, policymaking involves policymakers and influencers spread across many authoritative ‘venues’, with each venue having its own rules, networks, and ways of thinking.
In that context, policy theories identify the importance of contestation between policy actors, and describe the development of policy problems, and how evidence fits in. Approaches include:
The study of framing
The acceptability of a policy solution will often depend on how the problem is described. Policymakers use evidence to reduce uncertainty, or a lack of information around problems and how to solve them. However, politics is about exercising power to reduce ambiguity, or the ability to interpret the same problem in different ways.
By suggesting MUP would solve problems around crime, the UK Government made it easier for opponents to claim the policy wasn’t evidence-based. In Scotland, policymakers and advocates focused on health, where the evidence was stronger. In addition, the SNP’s approach fitted within a wider political independence frame, in which more autonomy meant more innovation.
The Narrative Policy Framework
Policy actors tell stories to appeal to the beliefs (or exploit the cognitive shortcuts) of their audiences. A narrative contains a setting (the policy problem), characters (such as the villain who caused it, or the victim of its effects), plot (e.g. a heroic journey to solve the problem), and moral (e.g. the solution to the problem).
Supporters of MUP tended to tell the story that there was an urgent public health crisis, caused largely by the alcohol industry, and with many victims, but that higher alcohol prices pointed to one way out of this hole. Meanwhile opponents told the story of an overbearing ‘nanny state’, whose victims – ordinary, moderate drinkers – should be left alone by government.
Social Construction and Policy Design
Policymakers make strategic and emotional choices, to identify ‘good’ populations deserving of government help, and ‘bad’ populations deserving punishment or little help. These judgements inform policy design (government policies and practices) and provide positive or dispiriting signals to citizens.
For example, opponents of MUP rejected the idea that alcohol harms existed throughout the population. They focused instead on dividing the majority of moderate drinkers from irresponsible minority of binge drinkers, suggesting that MUP would harm the former more than help the latter.
Multi-centric policymaking
This competition to frame policy problems takes place in political systems that contain many ‘centres’, or venues for authoritative choice. Some diffusion of power is by choice, such as to share responsibilities with devolved and local governments. Some is by necessity, since policymakers can only pay attention to a small proportion of their responsibilities, and delegate the rest to unelected actors such as civil servants and public bodies (who often rely on interest groups to process policy).
For example, ‘alcohol policy’ is really a collection of instruments made or influenced by many bodies, including (until Brexit) European organisations deciding on the legality of MUP, UK and Scottish governments, as well as local governments responsible for alcohol licensing. In Scotland, this delegation of powers worked in favour of MUP, since Alcohol Focus Scotland were funded by the Scottish Government to help deliver some of their alcohol policy goals, and giving them more privileged access than would otherwise have been the case.
The role of evidence in MUP
In the case of MUP, similar evidence was available and communicated to policymakers, but used and interpreted differently, in different centres, by the politicians who favoured or opposed MUP.
In Scotland, the promotion, use of, and receptivity to research evidence – on the size of the problem and potential benefit of a new solution – played a key role in increasing political momentum. The forms of evidence were complimentary. The ‘hard’ science on a potentially effective solution seemed authoritative (although few understood the details), and was preceded by easily communicated and digested evidence on a concrete problem:
- There was compelling evidence of a public health problem put forward by a well-organised ‘advocacy coalition’ (see below) which focused clearly on health harms. In government, there was strong attention to this evidence, such as the Lancet chart which one civil servant described as ‘look[ing] like the north face of the Eiger’. There were also influential ‘champions’ in Government willing to frame action as supporting the national wellbeing.
- Reports from Sheffield University appeared to provide robust evidence that MUP could reduce harm, and advocacy was supported by research from Canada which suggested that similar policies there had been successful elsewhere.
Advocacy in England was also well-organised and influential, but was dealing with a larger – and less supportive – Government machine, and the dominant political frame for alcohol harms remained crime and disorder rather than health.
Debates on MUP modelling exemplify these differences in evidence communication and use. Those in favour appealed to econometric models, but sometimes simplifying their complexity and blurring the distinction between projected outcomes and proof of efficacy. Opponents went the other way and dismissed the modelling as mere speculation. What is striking is the extent to which an incredibly complex, and often poorly understand, set of econometric models – and the ’Sheffield Model’ in particular – came to occupy centre stage in a national policy debate. Katikireddi and colleagues talked about this as an example of evidence as rhetoric:
- Support became less about engagement with the econometric modelling, and more an indicator of general concern about alcohol harm and the power of the industry.
- Scepticism was often viewed as the ‘industry position’, and an indicator of scepticism towards public health policy more broadly.
2. Who influences policy change?
Advocacy plays a key role in alcohol policy, with industry and other actors competing with public health groups to define and solve alcohol policy problems. It prompts our attention to policy networks, or the actors who make and influence policy.
According to the Advocacy Coalition Framework:
People engage in politics to turn their beliefs into policy. They form advocacy coalitions with people who share their beliefs, and compete with other coalitions. The action takes place within a subsystem devoted to a policy issue, and a wider policymaking process that provides constraints and opportunities to coalitions. Beliefs about how to interpret policy problems act as a glue to bind actors together within coalitions. If the policy issue is technical and humdrum, there may be room for routine cooperation. If the issue is highly charged, then people romanticise their own cause and demonise their opponents.
MUP became a highly charged focus of contestation between a coalition of public health advocates, who saw themselves as fighting for the wellbeing of the wider community (and who believed fundamentally that government had a duty to promote population health), and a coalition of industry actors who were defending their commercial interests, while depicting public health policies as illiberal and unfair.
3. Was there a ‘window of opportunity’ for MUP?
Policy theories – including Punctuated Equilibrium Theory – describe a tendency for policy change to be minor in most cases and major in few. Paradigmatic policy change is rare and may take place over decades, as in the case of UK tobacco control where many different policy instruments changed from the 1980s. Therefore, a major change in one instrument could represent a sea-change overall or a modest adjustment to the overall approach.
Multiple Streams Analysis is a popular way to describe the adoption of a new policy solution such as MUP. It describes disorderly policymaking, in which attention to a policy problem does not produce the inevitable development, implementation, and evaluation of solutions. Rather, these ‘stages’ should be seen as separate ‘streams’. A ‘window of opportunity’ for policy change occurs when the three ‘streams’ come together:
- Problem stream. There is high attention to one way to define a policy problem.
- Policy stream. A technically and politically feasible solution already exists (and is often pushed by a ‘policy entrepreneur’ with the resources and networks to exploit opportunities).
- Politics stream. Policymakers have the motive and opportunity to choose that solution.
However, these windows open and close, often quickly, and often without producing policy change.
This approach can help to interpret different developments in relation to Scottish and UK governments:
Problem stream
- The Scottish Government paid high attention to public health crises, including the role of high alcohol consumption.
- The UK government paid often-high attention to alcohol’s role in crime and anti-social behaviour (‘Binge Britain’ and ‘Broken Britain’)
Policy stream
- In Scotland, MUP connected strongly to the dominant framing, offering a technically feasible solution that became politically feasible in 2011.
- The UK Prime Minister David Cameron’s made a surprising bid to adopt MUP in 2012, but ministers were divided on its technical feasibility (to address the problem they described) and its political feasibility seemed to be more about distracting from other crises than public health.
Politics stream
- The Scottish Government was highly motivated to adopt MUP. MUP was a flagship policy for the SNP; an opportunity to prove its independent credentials, and to be seen to address a national public health problem. It had the opportunity from 2011, then faced interest group opposition that delayed implementation.
- The Coalition Government was ideologically more committed to defending commercial interests, and to framing alcohol harms as one of individual (rather than corporate) responsibility. It took less than a year for the alcohol industry to successfully push for a UK government U-turn.
As a result, MUP became policy (eventually) in Scotland, but the window closed (without resolution) in England.
Further Reading
Nicholls, J. and Greenaway, J. (2015) ‘What is the problem?: Evidence, politics and alcohol policy in England and Wales, 2010–2014’, Drugs: Education, Prevention and Policy 22.2 https://doi.org/10.3109/09687637.2014.993923
Paul Cairney and Donley Studlar (2014) ‘Public Health Policy in the United Kingdom: After the War on Tobacco, Is a War on Alcohol Brewing?’ World Medical and Health Policy, 6, 3, 308-323 PDF
Niamh Fitzgerald and Paul Cairney (2022) ‘National objectives, local policymaking: public health efforts to translate national legislation into local policy in Scottish alcohol licensing’, Evidence and Policy, https://doi.org/10.1332/174426421X16397418342227, PDF
Podcast
You can listen directly here:
You can also listen on Spotify or iTunes via Anchor

Using policy theories to interpret public health case studies: the example of a minimum unit price for alcohol – Understanding Public Policy (in 1000 and 500 words)
- Using policy theories to interpret public health case studies: the example of a minimum unit price for alcohol
- Policy in 500 Words: policymaking environments and their consequences
- Policy in 500 Words: bounded rationality and its consequences
- Policy in 500 Words: evolutionary theory
- Policy in 500 Words: The Advocacy Coalition Framework






Not commented on – but of interest – is the fact that Minimum Unit Pricing came into effect in Wales also in 2020 https://gov.wales/minimum-unit-pricing-alcohol?msclkid=ee42d16bbc0011eca79768ca67079e8c
Pingback: Why is there high support for, but low likelihood of, drug consumption rooms in Scotland? | Paul Cairney: Politics & Public Policy